Abdullah D Alanazi1,
Mohamed S Alyousif2 ![]() ,
Muheet A Saifi2,
Ibrahim O Alanazi3
,
Muheet A Saifi2,
Ibrahim O Alanazi3
For correspondence:- Mohamed Alyousif Email: msaifi@ksu.edu.sa Tel:+966114675777
Received: 22 April 2016 Accepted: 4 November 2016 Published: 22 December 2016
Citation: Alanazi AD, Alyousif MS, Saifi MA, Alanazi IO. Epidemiological studies on cutaneous leishmaniasis in Ad-Dawadimi District, Saudi Arabia. Trop J Pharm Res 2016; 15(12):2709-2712 doi: 10.4314/tjpr.v15i12.24
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To assess the prevalence of cutaneous leishmaniasis (CL) in Ad-Dawadimi region of Saudi Arabia.
Methods: Data from the patients included in this retrospective study were collected from the Leishmaniasis Control Center of Ad-Dawadimi District of Saudi Arabia. A total of 370 patients with CL were recorded from January 2009 to December 2013. The data focused on details of socio-demographics, i.e., age, gender, date of diagnosis, residence and close family members with CL.
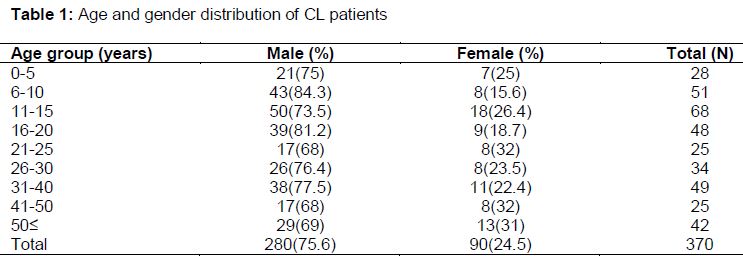
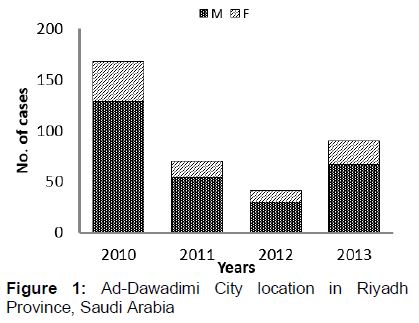
Results: Out of 370 patients with verified lesions, 280 (75.6 %) were males with a mean age of 18.26 ± 13.41 years, while 90 (24.3 %) were females with a mean age of 19.25 ± 16.10 years. The highest proportion (18.3 %) occurred in the 15 - 20 years age group. Annual distribution of CL showed that the highest rate was in 2010 with 168 cases while the lowest rate was in 2012 with 42 cases. There were no significant differences in the mean ages of the CL cases with respect to gender.
Conclusion: Most of the reported cases had with single facial lesions. Although all age groups are affected by CL, a majority of the cases are aged 15 to 30 years.
Introduction
Leishmaniasis is a complex disease of various clinical manifestations caused by infection with the protozoan parasites Leishmania spp. It is transmitted through bites from infected sand flies (Phlebotomus or Lutzomyia spp). Globally, there are an estimated 1.5 – 2 million new cases and 70000 deaths each year, and 350 million people are at risk of infection by the disease. Leishmaniasis-induced morbidity and mortality cause an estimated 2.4 million disability-adjusted life years [1].
Cutaneous leishmaniasis is endemic in the Eastern Province of Saudi Arabia, mainly in the Al-Hassa Oasis. The vector of the disease in Saudi Arabia is the sand fly and the alternative natural hosts are desert rodents. Leishmania tropica, the causative agent of cutaneous leishmaniasis in the Al-Hassa Oasis, classically causes skin lesions without dissemination. The main vector for L. tropica is Phlebotomus sergenti [2].
The present study was aimed at determining the prevalence of cutaneous leishmaniasis in Ad-Dawadimi region of Saudi Arabia.
Methods
Study site
Ad-Dawadimi is located on top of Najd Hill in the central area of Saudi Arabia. It is about 280 km west of Riyadh, the capital city of Saudi Arabia and is geographically located at latitude 24° North and longitude 44° East. The population of Ad-Dawadimi is approximately 240,000 thousand people. According to the Open Street Map project, Ad-Dawadimi has very hot summer up to 49 °C or more with an average temperature of 44 °C. Winter is very cold with temperature of 15 °C and windy nights. The overall climate is arid, receiving very little rainfall of 21.4 mm with relative humidity ranging from 12 to 50 % throughout the year.
Data collection
The data used in this retrospective study were from the Leishmaniasis Control Center of Ad-Dawadimi district. The Center was established in 2009. A total of 370 patients with CL were recorded from January 2009 to December 2013. Suspected cases of CL are referred from the primary health center to the specialized clinic where clinical examination and laboratory investigations were carried out. Samples were further examined microscopically at the central laboratory of Leishmania Control Unit (Directorate of Health, Ad Dawadimi).
The case investigation form included details of socio-demographics such as age, gender, nationality, date of diagnosis, residence and referral health center. Clinical data included methods of diagnosis (clinical examination and microscopic examination), localization of the lesions and treatment received (type, dose, route and duration). Consent was taken from the hospital authority as well as parents. School authority permitted and parents agreed for given research while written permission was also taken from the institutional ethical committee and the studies followed international guidelines [3]
Statistical analysis
Data analyses were performed using SPSS software version 16.0, for Windows, (Sydney, Australia), as well as Students t-test.
Results
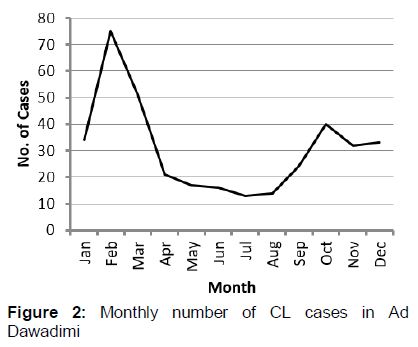
In all, data from 370 patients with lesions were collected. Data analysis showed that 75.6 % of patients were male (with a mean age of 18.26 ± 13.41 years), whereas 90 (24.3 %) patients were female (with a mean age of 19.25 ± 16.10 years). There were no significant differences in mean ages with respect to (). The youngest patient was 6 months of age and the oldest was 72 years. The mean age was 19.25 ± 14.77 years. The annual distribution of the cases showed that the highest incidence was in 2010 with 168 cases, and the lowest was in 2012 with 42 cases. The highest yearly incidence of CL was 1.68 per 10 000 in 2010 and the lowest was 0.42 per 10 000 in 2012 (). CL cases showed seasonal variations. The incidence steadily began to increase in October, peaked in February, and decreased to minimum in July - August ().
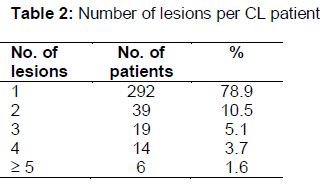
A total of 292 (78.9 %) patients had one lesion; 39 patients (10.5 %) had 2 lesions while 19, 14 and 6 patients had 3, 4 and more than 5 lesions respectively (). CL was located mostly on the exposed parts of the body such as face (197, 53.2 %); upper limb (109, 29.4 %) and lower limb (64, 17.2 %).
Discussion
The purpose of this study was to assess epidemiological data of reported CL cases in Leishmaniasis Control Center of Ad-Dawadimi district Saudi Arabia. CL is a parasitic disease caused by the protozoa of the genus Leishmania such as L. tropica, L. major, L. aethiopica, and sometimes L. donovani and L. infantum. The infection is transmitted through small phlebotomine sand flies when they bite infected human or animal hosts. Clinical characteristics of leishmaniases depend on Leishmania parasite invasiveness, tropism, pathogenicity, and immune responses of the host [4-6]. Majority of the CL cases presented with single facial lesions. These finding are similar to those of Al-Tawfiq and Abu Khamsin [7]. Most recent epidemiological studies in Yemen, Saudi Arabia and Israel revealed a similar trend, with single lesions on the face or limbs being the most common form of presentation [7,9-12].
Al-Tawfiq and Abu Khamsin [7] had conducted a very comprehensive 46-year study on Leishmania cases in Saudi Arabia. They showed that CL had a very high incidence, almost reaching epidemic proportions in 1973 and thereafter declining to a plateau in the mid-1980s. The results of this study confirm the downward trend in incidence of CL, showing a clear decline especially during the period 2010-2014. A similar downward trend for the incidence was studied by Amin et al [2].
The seasonal incidence of CL seen in this study is similar to that of a previous study [2], which reported that the incidence increased in September and reached a peak in January/February. This might be related to the activity of the vector. In general, CL tended to affect the younger age group in most endemic areas. In two previous studies [2,4- 7], majority of the cases occurred in people aged less than 15 - 20 years. This is similar to findings in other studies [10,13,14]. Although all age groups were affected by CL, majority of them were between 15-30 years old. The reason for low CL incidence among elderly patients may be related to the fact that they were infected during early ages and so acquired long-term immunity. Another factor is that older people do not care to visit a health center for the treatment of CL. Although they know about this disease, its disfiguring scars does not seem to bother them as much as it bothers youngsters. In addition, young people are more involved in outdoor activities which expose them more to the disease than older age groups. In our the present study, the lesions were found most frequently on the face; this is consistent with reports by Şanlıurfa and Adana [15,16].
Conclusion
Majority of the reported cases of CL are those with single facial lesions. Although all age groups are affected by CL, most of the cases lie in the 15 - 30 years age group. There were no significant differences among the age groups with respect to gender.
Declarations
Acknowledgement
References
Archives


News Updates